Annals of Neurosciences, Vol 17, No 2 (2010)
Annals of Neurosciences, Volume 17, Issue 2 (April), 2010
The current status of gene therapy for Parkinson's disease
ABSTRACT
The recent development of viral vectors, especially vectors derived from adeno-associated virus (AAV), has translated gene therapy for Parkinson's disease (PD) from animal experiments into clinical trials. The current gene therapy protocols used are based on three major strategies. The first protocol involves local production of dopamine via the introduction of dopamine-synthesizing enzyme genes into the putamen. The aromatic L-amino acid decarboxylase (AADC) gene has been transferred in this manner with the aim of efficiently converting orally administered L-dopa. The delivery of triple genes including tyrosine hydroxylase (TH), guanosine triphosphate cyclohydrolase I (GCH) and AADC is also being undertaken, and is aimed at continuously supplying dopamine into the putamen. The second protocol involves the protection of nigrostriatal projections via the production of neurturin, a trophic factor for dopaminergic neurons in the putamen. The final method includes the modulation of neural activity along the output pathway of the basal ganglia by transducing the subthalamic nucleus with vectors expressing glutamic acid decarboxylase (GAD-65, GAD-67), a key enzyme required for the synthesis of the inhibitory transmitter -aminobutyric acid (GABA). The initial results of phase 1 studies using AAV vectors have not only confirmed the safety of these vectors, but have also revealed the alleviation of motor symptoms associated with PD.
KEY WORDS: Adeno-associated virus, Aromatic L-amino acid decarboxylase, Neurturin, Glutamic acid decarboxylase, Positron emission tomography
Corresponding Author: Shin-ichi Muramatsu, M.D, Ph.D, E-mail : muramats@jichi.ac.jp; Tel: +81-285-58-7352, Fax: +81-285-44-5118
doi : 10.5214/ans.0972-7531.1017209
Introduction
Almost two decades have passed since the first gene therapy clinical trial was conducted for the treatment of adenosine deaminase deficiency at the National Institute of Health in the United States in 1990. Although gene therapy appeared to be a ground breaking form of medical treatment at the time, it has not proven to be as successful in treating disease as initially anticipated. A patient with ornithine transcarbamylase deficiency died of systemic inflammatory response syndrome (SIRS) following the administration of a large quantity of adenoviral vector into the hepatic artery.1 In addition, some children with X–linked severe combined immunodeficiency (X–SCID) developed leukemia due to the activation of an oncogene after gene therapy using a retroviral vector.2,3 These reports describing the severe, adverse effects of gene therapy dampened the excitement underlying the success of gene therapy treatment to some extent. However, encouraging results have been obtained more recently with clinical studies for Parkinson's disease (PD).4-7
| Gene | AADC | TH/GCH/AADC | Neurturin | GAD | ||||
| Function | Convert L-dopa to dopamine | Synthesis of dopamine from tyrosine | Neurotrophic factor for dopaminergic neurons | Synthesis of inhibitory neurotransmitter GABA | ||||
| Vector | AAV | EIAV | AAV | AAV | ||||
| Phase | I | I | I | II | I | II | ||
| Institute | UCSF7 | JMU | Henri Mondor Hospital22 | UCF6 | Multi-center26 | NYP Hospital5 | Multi-center | |
| Dose | 9x1010 3x1011 |
3x1011 |
1x 2x |
1.3x1011 5.4x1011 |
5.4x1011 Sham |
3.5x109 1x1010 3.5x1010 |
1x1011 Sham |
|
| Number of subjects | 10 | 6 | 6 | 12 | 54 | 12 | 40 | |
| Target | Putamen (Bilateral) |
Putament (Bilateral) |
Putamen (Bilateral) |
STN (Unilateral) |
STN (Bilateral) |
|||
| PET tracer | [18F] fluro-m-tyrosine | [18F] fluro-DOPA | [18F] fluro-deoxyglucase | |||||
AADC, aromatic L-amino acid decarboxylase; AAV, adeno-associated virus; EIAV, equine infectious anemia virus; GABA, γ-aminobutyric acid; GAD, glutamic acid decarboxylase; GCH, guanosine triphosphate cyclohydrolase I; TH, tyrosine hydroxylase; STN, subthalamic nucleus. Dose of AAV vectors are represented as vector genome/patient.
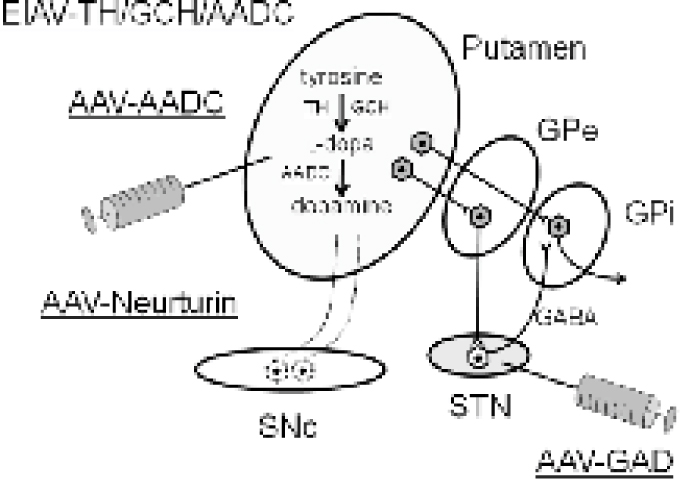
Figure. Current gene therapy strategies for the treatment of Parkinson's disease
Three gene therapy strategies are currently available for the treatment of (PD. 1) production of dopamine. AAV vectors expressing AADC or EIAV vector expressing TH, GCH and AADC are infused into the putamen. 2) Protection of the nigrostriatal pathway. The neurotrophic factor neurturin is produced continuously in the putamen. 3) Modification of neuronal activity in the STN by introducing the GAD gene.
AADC, aromatic L-amino acid decarboxylase; AAV, adeno-associated virus; EIAV, equine infectious anemia virus; GABA, γ-aminobutyric acid; GAD, glutamic acid decarboxylase; GCH, guanosine triphosphate cyclohydrolase I; GPe, globus pallidus external segment; GPi, globus pallidus internal segment; TH, tyrosine hydroxylase; SNc, substantia nigra pars compacta; STN, subthalamic nucleus.
Adeno-associated virus vectors
Technology that efficiently introduces a therapeutic gene into target cells is essential for successful gene therapy. Viral vectors, in particular vectors derived from adeno–associated virus (AAV), have been shown to be suitable for the transduction of neurons in the mammalian brain using stereotaxic surgery.8 AAVs are small (25 nm), single stranded DNA viruses that belong to Parvoviridae.9 No clear pathogenicity in humans has been reported, and many adults synthesize antibodies against AAVs following latent infection in childhood.10,11 The AAV genome exists in episomes in the nucleus and is rarely incorporated in the chromosomes. To date, more than one hundred genotypes have been defined for primate AAVs. The vast majority of vectors used in clinical applications are derived from serotype 2 (AAV2).
AAV2 has a 4.7–kb genome, both ends of which contain hairpin structures called inverted terminal repeats (ITR). A region encoding the non–structural protein Rep and capsid protein VP are also present. These regions for Rep and VP can be substituted with a therapeutic gene when constructing vectors. AAV vectors express an exogenous gene in the brain for long term use (more than seven years) and do not produce any significant inflammatory or immuno–logical reactions.12 Although the size of the genes that can be inserted into the AAV2 genome is limited to less than 4.5 kb, most of the therapeutic genes fit into this range. It has also been shown that several AAV vectors are able to infect one cell at the same time and can express plural genes. 13 AAV vectors have been applied in clinical trials for numerous disorders including hemophilia,14 cystic fibrosis15and retinal degeneration.16 To date, adverse effects due to the administration of the vectors themselves have not been found. In addition to gene therapy, AAV vectors have also been recently used as a genetic tool in the neurosciences.17,18
Gene transfer of dopamine–synthesizing enzymes
Dopamine is synthesized in the brain from diet–derived L–tyrosine. Three enzymes are essential in this production process.19 Tyrosine hydroxylase (TH) is the rate–limiting enzyme that converts L–tyrosine to L–3, 4–dihydroxy–phenyla–lanine (L–dopa). Guanosine triphosphate cyclohydrolase I (GCH) is the rate–limiting enzyme that synthesizes the essential TH co–factor tetrahydrobiopterine (BH4), while aromatic L–amino acid decarboxy–lase (AADC) converts L–dopa to dopamine. These three enzymes are transported from the substantia nigra in an anterograde manner to the striatum. A severe loss of the nerve terminals in advanced Parkinson's disease (PD) is associated with an 80–95% depletion of striatal enzyme activity. Gene transfer of TH, GCH and AADC,13,20 or AADC alone,12,21 into the striatal neurons has led to behavioral recovery in primate models of PD.
Two phase I clinical trials were conducted at the University of California San Francisco (UCSF) and Jichi Medical University (JMU) to evaluate the safety and potential efficacy of AAV vector–mediated gene delivery of AADC to the bilateral putamen. Alleviation of motor symptoms associated with PD was observed in both trials. In the UCSF study,7 a low dose cohort of five patients received 11011 vector genome (vg) and a high dose cohort of five patients received 31011 vg of AAV–AADC. The mean improvements of the ten patients in the total score of unified Parkinson's disease rating scale (UPDRS) were 31% (10.5 points) in the off–state and 32% (10 points) in the on–state. The mean improvements in the motor score of UPDRS were 36% (12 points) in the offstate and 28% (4.3 points) in the on–state. Positron emission tomography (PET) using [18F]fluoro–m–tyrosine (FMT), a tracer for AADC, revealed a 30 and 75% increase in Kk values in the putamen of the low–dose and high–dose cohort, respectively, at 6 months after the gene delivery. In the JMU study, six patients received 31011 vg of AAV–AADC. Motor function in the off–state improved to a mean of 46% (11.6 points) based on the UPDRS scores at six months after surgery, without any apparent changes in the short–duration response to levodopa. PET revealed a 56% increase in FMT activity, which persisted for up to 96 weeks (manuscript in preparation). Phase 2 trials of AAV–AADC are currently in the planning stages.
Using a vector derived from the equine infectious anemia virus (EIAV), a type of lentivirus, a phase I/II trial involving the triple gene transfer of TH, GCH and AADC into the bilateral putamen has been initiated at the Henri Mondor Hospital in France.22 Two dose levels have been evaluated in cohorts of three patients per dose. All patients treated at the second dose level have completed their six–month assessments and have shown improvement in motor function in the off–state when evaluated on the motor score of UPDRS. The mean improvement was 34% relative to the patients' pre– treatment motor function.22 Studies into the high dose (5 times the lower dose) cohort are planned. Using this triple gene transfer, dopamine will be continuously produced in the putamen and may reduce “wearing–off” effects by avoiding pulsatile stimulation of dopaminergic receptors.
Gene transfer of neurturin
An alternative approach to gene therapy for PD is the protection of the nigrostriatal pathways from progressive degeneration by providing genes encoding for neurotrophic factors. Neurturin is a natural analog of glial cell line–derived neurotrophic factor (GDNF).23 GDNF is a small glycoprotein that provides strong trophic support for the dopaminergic neurons. However, GDNF protein has limited usefulness as a therapeutic agent due to its short duration of activity and poor ability to cross the blood–brain barrier. In animal models of neurotoxin induced PD, viral vector–mediated gene delivery halts ongoing degeneration of the nigrostriatal pathway, resulting in functional recovery, even after substantial numbers of dopaminergic cells have been depleted.24,25
A phase I gene therapy trial that introduced the neurturin gene into the bilateral putamen was conducted at the UCSF6. The first six patients entered into the study receiving a dose of 31011 vg, while the next six patients received a dose of 5.41011 vg of AAV vector. A mean improvement of 36% (14 points) in the UPDRS motor score in the off–state and a mean increase of 25% (2.3 h) in on time without troublesome dyskinesia were observed one year after surgery. Subsequently, a phase II double–blind control study was undertaken at nine academic institutions in the United States, and in which one–third of a total of 54 patients received sham surgery (partial burr hole without infusion of vectors). Significant differences were not obtained in terms of the degree of motor performance between the gene transfer group and the control group at 12 months, although some treatment effects have since been observed in 30 subjects followed for 18 months under blind conditions.26 Analysis of postmortem brain tissue from two patients treated with AAV vectors demonstrated that neurturin was expressed in the putamen, but not in the substantia nigra. Earlier intervention may be required for success in future trials of this kind of neuro–protective approach, as most of the nigrostriatal fibers have already been lost when the PD symptoms appear.
Gene transfer of glutamic acid decarboxylase
In PD, depletion of dopamine in the striatum leads to an increase in the activity of the subthalamic nucleus (STN).27 The increased excitatory drive of the STN to the internal portion of the globus pallidus (GPi) and to the substantia nigra pars reticulata (SNr) then exerts inhibitory effects on the thalamo–cortical projection and brainstem nucleus, resulting in motor symptoms such as bradykinesia and rigidity. During the last two decades, deep brain stimulation of the STN, which is thought to modify STN output by high–frequency stimulation, has become routine treatment for advanced PD patients and has resulted in the improvement of motor function. Gene transfer of glutamic acid decarboxylase (GAD–65 and GAD–67), a rate–limiting enzyme required for the synthesis of inhibitory transmitter ?–aminobutyric acid (GABA), into the STN is aimed at converting excitatory output to inhibitory output, thus, obtaining a similar effect to electrical stimulation.28
An open–label phase I clinical trial has been conducted at the New York Presbyterian Hospital.5 A total of 12 patients in three dose–escalation cohorts received AAV–GAD into the unilateral STN contra–lateral to more severe motor symptoms. At 12 months after the vector infusion, the mean improvement on motor score of UPDRS was 27% in the offstate and 24% in the on–state.5 A PET scan using [18F]fluorodeoxyglucose (FDG) as a tracer revealed a decrease in uptake into the ventrolateral nucleus (VL) and dorsomedial nucleus (MD) of the thalamus on the operated side, and an increased uptake in the ipsilateral premotor and motor cortical regions.29
The underlining physiological changes in PD include, in addition to increases in the firing rate of the STN, the tendency of pallidal neurons to fire in more irregular patterns, as well as abnormal oscillatory synchronization in the basal ganglia.30Thus, mechanisms underlying how DBS and AAV–GAD gene therapy is effective remain to be defined.31 A double–blinded phase II study of AAV–GAD infusion into the bilateral STN is currently underway for 40 subjects, including 20 subjects that received sham surgery.
Future prospects
Owing to the development of efficient viral vectors, gene therapy for PD has been tested in clinical trials, with the initial results of phase I studies proving encouraging. In contrast to cell transplantation, immunosuppressive drugs are not necessary for the current gene therapy strategies. If the primary purpose of treatment is the supplementation of dopamine into the striatum for improving motor performance, then gene therapy appears to be simpler than cell transplants. Cell therapy may prove useful in treating Parkinsonism including cerebral ischemia, striato–nigral degeneration and cortico–basal degeneration, where neurons in the striatum are damaged. However, several PD symptoms that L–dopa is not effective at rescuing including cognitive dysfunction, depressive state, frozen gait, posture reflex disturbance and sleep disturbance have also been reported. 32For the treatment of these symptoms, effective therapeutic genes must be identified and delivered into the appropriate areas of the brain. Development of vector constructs that avoid over–expression is also required for increasing safety.33 Although AAV and EIAV are reported to be non–pathogenic for humans, the long–term safety must be confirmed. It is expected that in the near future gene therapy will become the general choice for the treatment of PD.
Competing interests – None
Received Date : 13 February 2010
Revised Date : 7 June 2010
Accepted Date : 7 July 2010
References
1. Wilson JM, Lessons learned from the gene therapy trial for ornithine transcarba-mylase deficiency. Mol Genet Metab 2009; 96:151-7
2. Hacein-Bey-Abina S, Garrigue A, Wang GP, et al. Insertional oncogenesis in 4 patients after retrovirus-mediated gene therapy of SCID-X1. J Clin Invest 2008; 118:3132-42
3. Howe SJ, Mansour MR, Schwarzwaelder K, et al. Insertional mutagenesis combined with acquired somatic mutations causes leukemogenesis following gene therapy of SCID-X1 patients. J Clin Invest 2008; 118:3143-50
4. Kaplitt MG, Parkinson disease: Another player in gene therapy for Parkinson disease. Nat Rev Neurol 2010; 6:7-8
5. Kaplitt MG, Feigin A, Tang C, et al. Safety and tolerability of gene therapy with an adeno-associated virus (AAV) borne GAD gene for Parkinson's disease: an open label phase I trial. Lancet 2007; 369:2097-105
6. Marks WJ Jr., Ostrem JL, Verhagen L, et al. Safety and tolerability of intraputa-minal delivery of CERE-120 (adeno-associated virus serotype 2-neurturin) to patients with idiopathic Parkinson's disease: an open-label, phase I trial. Lancet Neurol 2008; 7:400-8
7. Christine CW, Starr PA, Larson PS, et al. Safety and tolerability of putaminal AADC gene therapy for Parkinson disease. Neurology 2009; 73:1662-9
8. Muramatsu S, Fujimoto F, Katoa S, et al. A phase 1 study of aromatic L-amino acid decarboxylase gene therapy for Parkinsons disease. Mol Ther 2010 in press.
9. Shen Y, Post L, Viral vectors and their applications. Knipe DM, Howley PM, ed. Fields' virology. Philadelphia. Lippincott Williams & Wilkins, 2006; 1:547-50
10. Boutin S, Monteilhet V, Veron P, et al. Prevalence of serum IgG and neutralizing factors against adeno-associated virus types 1, 2, 5, 6, 8 and 9 in the healthy population: implications for gene therapy using AAV vectors. Hum Gene Ther 2010 in press.
11. Ito T, Yamamoto S, Hayashi T, et al. A convenient enzyme-linked immunosorbent assay for rapid screening of anti-adeno-associated virus neutralizing antibodies. Ann Clin Biochem 2009; 46:508-10
12. Bankiewicz KS, Forsayeth J, Eberling JL, et al. Long-term clinical improvement in MPTP-lesioned primates after gene therapy with AAV-hAADC. Mol Ther 2006; 14:564-570
13. Shen Y, Muramatsu S, Ikeguchi K, et al. Triple transduction with adeno-associated virus vectors expressing tyrosine hydroxylase, aromatic L-amino acid decarboxylase, and GTP cyclohydro-lase I for gene therapy of Parkinson's disease. Hum Gene Ther 2000; 11:1509-19
14. Hasbrouck NC, High KA, AAV-mediated gene transfer for the treatment of hemophilia B: problems and prospects. Gene Ther 2008; 15:870-5
15. Mueller C, Flotte TR, Gene therapy for cystic fibrosis. Clin Rev Allergy Immunol 2008; 35:164-78
16. Maguire AM, High KA, Auricchio A, et al. Age-dependent effects of RPE65 gene therapy for Leber's congenital amaurosis: a phase 1 dose-escalation trial. Lancet 2009; 374:1597-605
17. Fukushima F, Nakao K, Shinoe T, et al. Ablation of NMDA receptors enhances the excitability of hippocampal CA3 neurons. PLoS One 2009; 4:e3993
18. Kadkhodaei B, Ito T, Joodmardi E, et al. Nurr1 is required for maintenance of maturing and adult midbrain dopamine neurons. J Neurosci 2009; 29:15923-32
19. Vinish M, Milstein J, Non-Motor aspects of Parkinso's disease. Annals of Neurosciences 2009; 16(4):176-179
20. Muramatsu S, Fujimoto K, Ikeguchi K, et al. Behavioral recovery in a primate model of Parkinson's disease by triple transduction of striatal cells with adeno-associated viral vectors expressing dopamine-synthesizing enzymes. Hum Gene Ther 2002; 13:345-54
21. Bankiewicz KS, Eberling JL, Kohutnicka M, et al. Convection-enhanced delivery of AAV vector in parkinsonian monkeys; in vivo detection of gene expression and restoration of dopaminergic function using pro-drug approach. Exp Neurol 2000; 164:2-14
22. Oxford Biomedica. Oxford Biomedica announces update on phase I/II study of ProSavin in Parkinson's disease and publication of preclinical results. Available from: http://www.oxford-biomedica.co.uk (15 October 2009).
23. Horger BA, Nishimura MC, Armanini MP, et al. Neurturin exerts potent actions on survival and function of midbrain dopaminergic neurons. J Neurosci 1998; 18:4929-37
24. Wang L, Muramatsu S, Lu Y, et al. Delayed delivery of AAV-GDNF prevents nigral neurodegeneration and promotes functional recovery in a rat model of Parkinson's disease. Gene Ther 2002; 9:381-9
25. McGrath J, Lintz E, Hoffer BJ, et al. Adeno- associated viral delivery of GDNF promotes recovery of dopaminergic phenotype following a unilateral 6-hydroxydopamine lesion. Cell Transplant 2002; 11:215-27
26. Ceregene. Ceregene presents additional clinical data from phase 2 trial of CERE-120 for Parkinson's disease. Available from: http://www.ceregene.com/ (May 27, 2009).
27. Obeso JA, Rodriguez-Oroz MC, Benitez-Temino B, et al. Functional organization of the basal ganglia: therapeutic implications for Parkinson's disease. Mov Disord 2008; 23 Suppl 3:S:548-59
28. During MJ, Kaplitt MG, Stern MB, et al. Subthalamic GAD gene transfer in Parkinson disease patients who are candidates for deep brain stimulation. Hum Gene Ther 2001; 12:1589-91
29. Feigin A, Kaplitt MG, Tang C, et al. Modulation of metabolic brain networks after subthalamic gene therapy for Parkinson's disease. Proc Natl Acad Sci USA 2007; 104:19559-64
30. Montgomery EB Jr., Basal ganglia pathophysiology in Parkinson's disease. Ann Neurol 2009; 65:618; author reply 618-9
31. Gradinaru V, Mogri M, Thompson KR, et al. Optical Deconstruction of Parkinsonian Neural Circuitry. Science 2009; 324:354-9
32. Sethi K, Levodopa unresponsive symptoms in Parkinson disease. Mov Disord 2008; 23 Suppl 3:S:521-33
33. Li XG, Okada T, Kodera M, et al. Viral-mediated temporally controlled dopamine production in a rat model of Parkinson disease. Mol Ther 2006; 13:160-6
(c) Annals of Neurosciences.All Rights Reserved